
 English
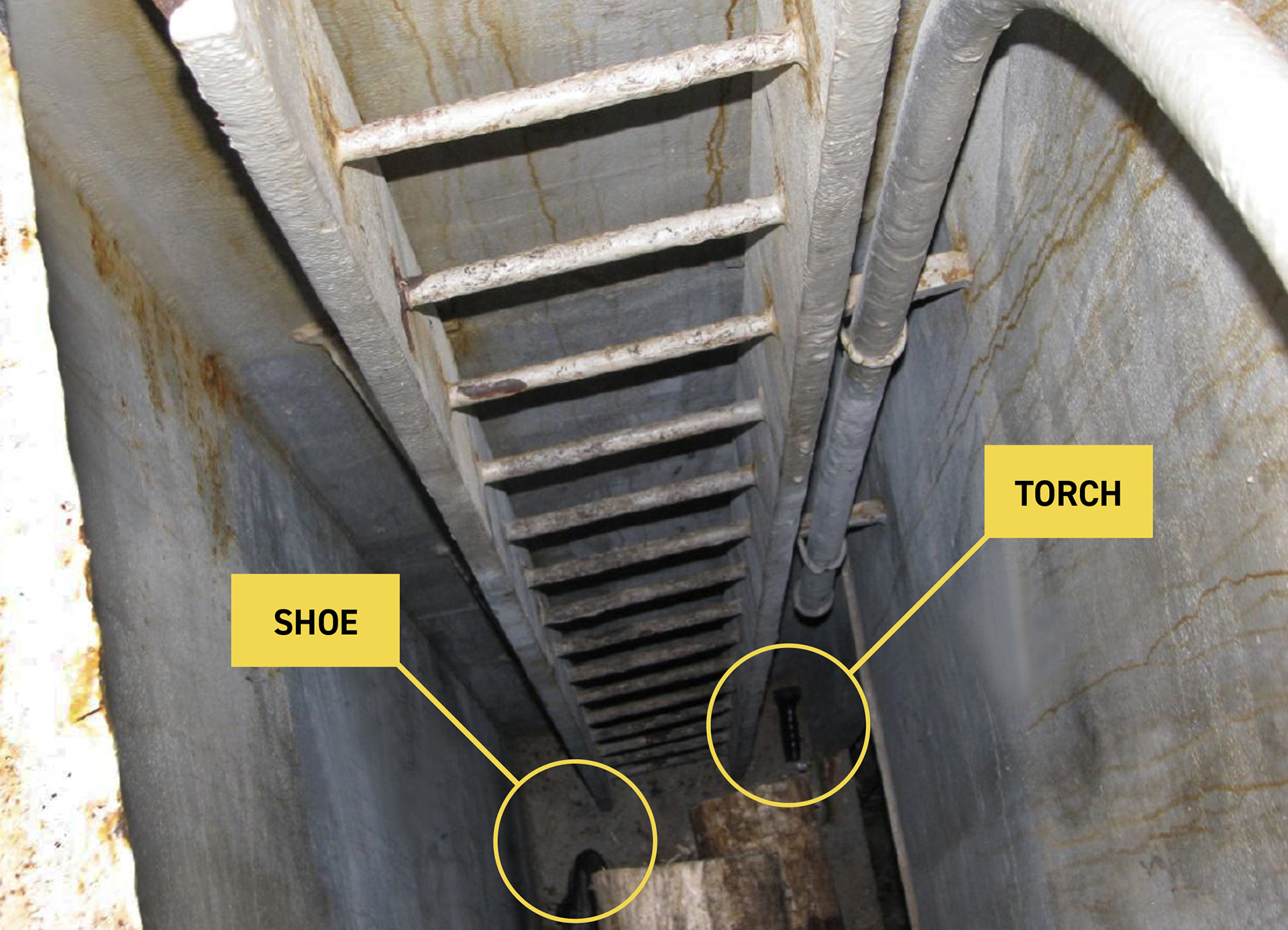
EnglishA bulk carrier was loading logs in Port Marsden, New Zealand (NZ), when the chief officer (C/O) entered a cargo hold which contained logs. Upon entry he rapidly lost consciousness and fell from the entrance ladder (Figure 1). A fellow crew member who tried to rescue the C/O suffered the same fate. They were later both pronounced dead due to asphyxia.
Source: Investigation report by the Transport Accident Investigation Commission, New Zealand
WHAT HAPPENED?
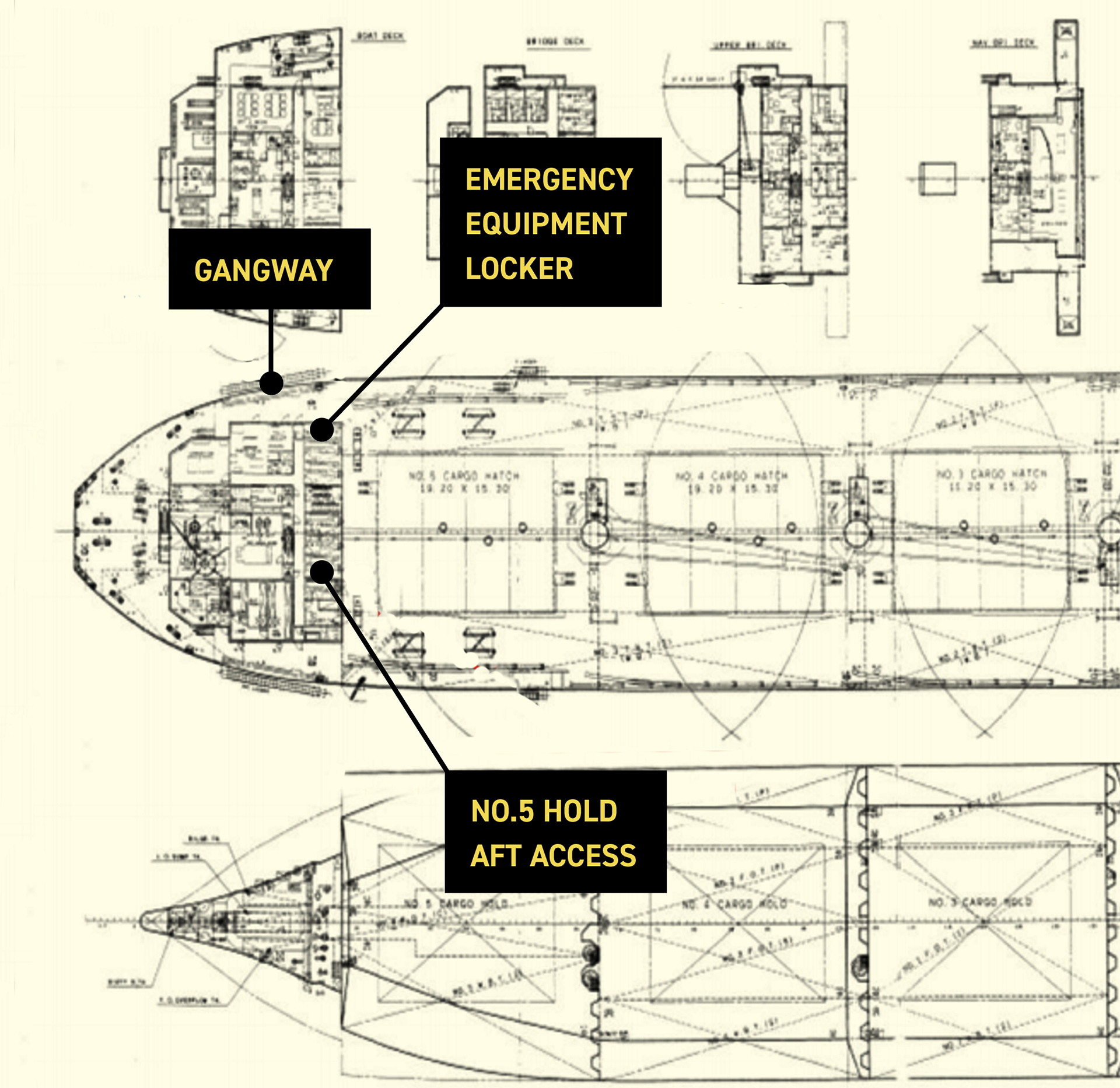
After loading logs at various ports in New Zealand the ship had arrived in Port Marsden, here another 11,476m3 of logs were loaded. The logs were to be fumigated on passage to China, and two fumigation officials embarked to carry out a pre-inspection. They reported to the master that hatches 1F to 4F had excessive amounts of water visible, which needed to be removed before fumigation could take place, and that the rubber seal on hold No. 5 aft access door (Figure 2) needed replacing.
The master discussed the matter with the C/O, who then proceeded on deck. He asked the bosun to follow him to hold No.5, where they opened the access hatch and the C/O climbed onto the ladder and started to descend. The bosun tried to follow, but after only a few steps the C/O suddenly fell onto the logs below. The bosun immediately alerted fellow crew members standing at the gangway, then made his way to the aft mooring station to get a rope to retrieve the C/O.
Source: Investigation report by the Transport Accident Investigation Commission, New Zealand
The second officer (2/O) was at the gangway and alerted the master by radio. He then fetched a breathing apparatus (BA) set and also oxygen from the ship’s hospital. An able seaman (AB) ran into the accommodation to alert the third officer (3/O) in the ship’s office, then tried to follow the AB to the incident site. However, the AB disappeared from view, so the 3/O instead went to hold No.4, where he met the master. Both were unsure of where the incident had occurred.
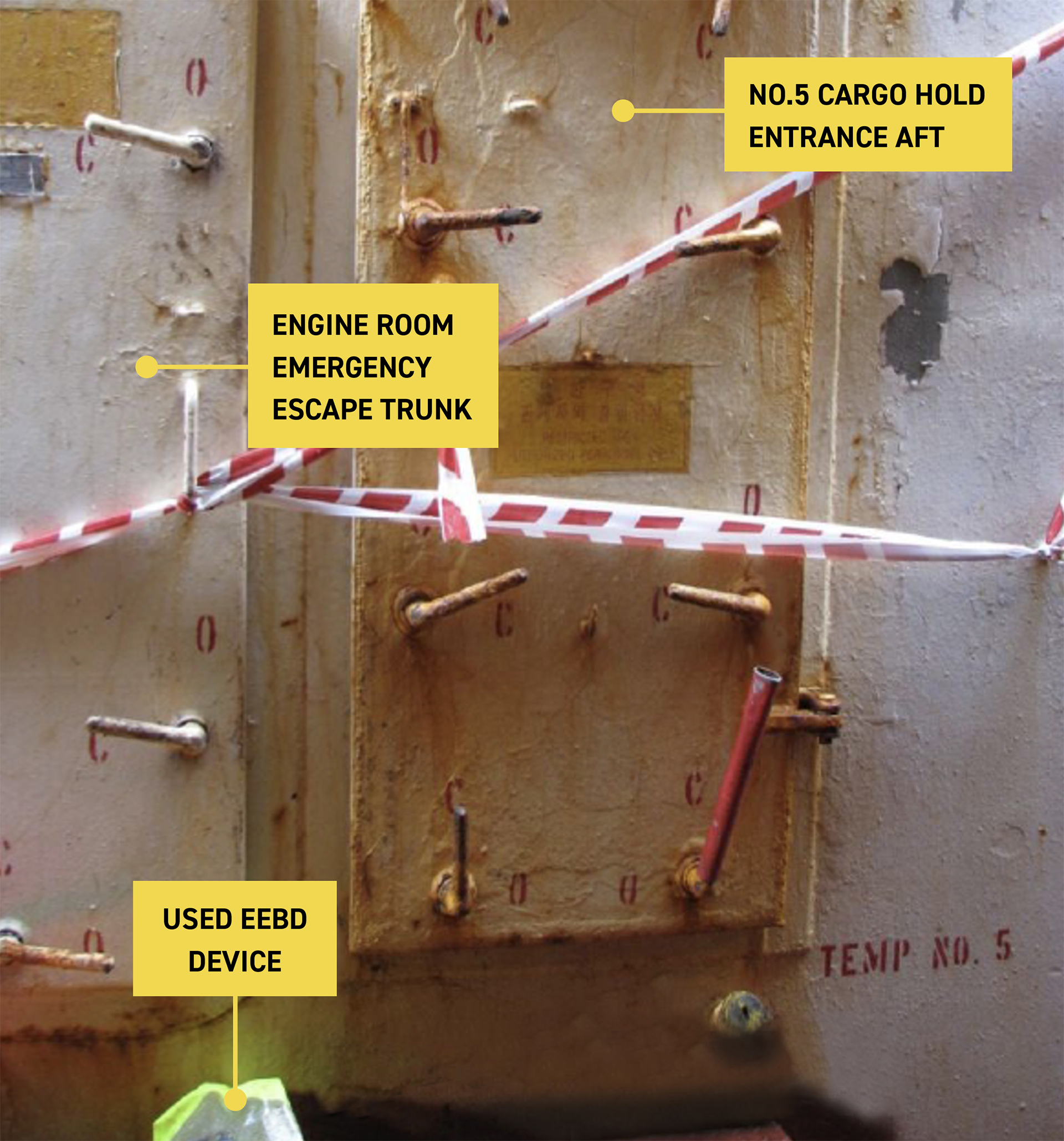
When returning to the access (Figure 3) the bosun found the AB, who had alerted the 3/O, climbing down into the hold with another crew member about to follow. The bosun managed to prevent the latter from entering but heard the AB fall. Looking down he noticed him lying, apparently unconscious, on top of the C/O.
The master arrived at the scene and instructed the 3/O to fetch a BA set. The master then went to the wheelhouse to activate the general alarm. On his way he informed the fumigation officials, who called the local emergency services to request an ambulance.
The 3/O returned and put on the BA set, tied the rescue rope around his waist and entered the hold. He was able to tie the rope around the C/O, who was then hauled onto deck
As the 3/O was too exhausted to attempt to rescue the AB, the first engineer (1/E), put on the other BA set and descended down to the hold. However, the BA set prevented him manoeuvring past a protruding log so he exited, and instead put on an emergency escape breathing device (EEBD), then re-entered. When he got to the AB, he noticed what he thought were signs of life. He took off his EEBD mask and placed it momentarily on the AB to try to revive him. He then replaced his mask and managed to attach the rescue rope to the AB, who was hauled onto deck. As the 1/E was nearing the top of the access ladder his EEBD ran low on compressed air, and he had to be hauled out. When he reached the upper deck, he was suffering from asphyxia.
Ambulance staff arrived and tried to resuscitate the C/O and the AB, but both were pronounced dead at the scene. The ambulance staff also administered oxygen to the 1/E, and he was airlifted to the nearest hospital.
Source: Investigation report by the Transport Accident Investigation Commission, New Zealand
Further details about the incident and the lessons learned are provided in the summary of the case study.
In addition, a presentation and reflective learning form have been prepared based on the incident as suggested training materials. These can be used by Members or their crew in any way they see fit to encourage reflection and gain the maximum learning from this incident: to consider why the incident happened; “what it means to me”, and to then relate the identified learning points to one’s own personal situation.
Finally, a Britannia commentary on the incident has been prepared which discusses the key points in more detail in order to help develop the reflective learning from the case study.
CASE STUDY MATERIAL
BSAFE INCIDENT CASE STUDY NO.5 – SUMMARY
BSAFE INCIDENT CASE STUDY NO.5 – REFLECTIVE LEARNING FORM
Lessons Learned
The following lessons learned have been identified. These are based on the information available in the investigation report and are not intended to apportion blame on the individuals or company involved:
- Testing of the hold atmosphere after the incident revealed that the oxygen level 3 metres down the ladder was as low as 3%.
- According to the autopsy reports, the C/O and the AB died from asphyxia due to oxygen deprivation, which was consistent with the depleted level of oxygen in the cargo hold.
- Oxygen levels in the cargo hold would have been depleted by organic decomposition of the logs, a phenomena well-known to the shipping industry.
- The ship’s safety management manual referred to the dangers associated with the cargo and the procedures to be taken if entering an enclosed space but these were not adhered to.
- Regular and effective enclosed space drills and training are key to ensuring awareness and preparedness. No evidence could be found of this during the previous 3 months.
- The investigation could not establish what enclosed space training the deceased AB had received.
- The reason why the experienced C/O ignored the bosun’s warnings and entered the hold could not be established. An effective Stop Work Authority program would have supported the bosun.
- The onboard rescue response was not well coordinated or practised. Given the survival time in the atmosphere, any rescue attempt would have had to have been immediate and efficient.
- EEBDs are designed only to be used while escaping a hazardous atmosphere and should not be used to enter an oxygen deficient space. This placed the 1/E at considerable risk.
For more information on this incident email lossprevention@tindallriley.com
THIS CASE STUDY IS DRAWN FROM THE INVESTIGATION REPORT 10-201 PUBLISHED BY THE TRANSPORT ACCIDENT INVESTIGATION COMMISSION, NEW ZEALAND.
THE PURPOSE OF THIS CASE STUDY IS TO SUPPORT AND ENCOURAGE REFLECTIVE LEARNING. THE DETAILS OF THE CASE STUDY MAY BE BASED ON, BUT NOT NECESSARILY IDENTICAL TO, FACTS RELATING TO AN ACTUAL INCIDENT. ANY LESSONS LEARNED OR COMMENTS ARE NOT INTENDED TO APPORTION BLAME ON THE INDIVIDUALS OR COMPANY INVOLVED. ANY SUGGESTED PRACTICES MAY NOT NECESSARILY BE THE ONLY WAY OF ADDRESSING THE LESSONS LEARNED, AND SHOULD ALWAYS BE SUBJECT TO THE REQUIREMENTS OF ANY APPLICABLE INTERNATIONAL OR NATIONAL REGULATIONS, AS WELL AS A COMPANY’S OWN PROCEDURES AND POLICIES.